Transcaval access for transcatheter aortic valve replacement: Use of Brockenbrough needle
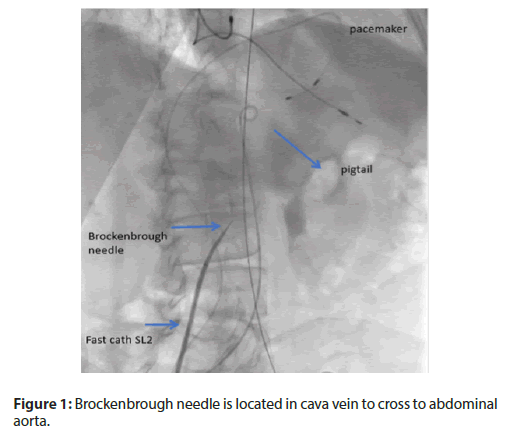
ranscaval access is a completely percutaneous route from the inferior cava vein, through the retroperitoneal interstitial space and into the abdominal aorta to allow therapeutic procedures, such as transcatheter aortic valve replacement. It is an alternative to access to the femoral artery when the iliofemoral arteries are too small or too diseased to accommodate the desired introducer sheath. Transcaval access to the aorta is based on the observation that the interstitial hydrostatic pressure exceeds the venous pressure. As a result, in the retroperitoneal space, blood that leaves the abdominal aortic returns to the venous circulation through a hole in the cava vein, instead of being accumulated as hemorrhage. This physiology allows the large transcave sheaths to be temporarily removed during tract repair and allows the aortocaval tracts to be closed with nitinol occluding devices [5]. The traditional transcaval access is described with the use of a rigid-tip coronary CTO guidewire, aided by microcatheter and electrocautery, which is advanced in a calcium-free target in the aorta. Then, the system is exchanged by stiff support guide and delivery system is advanced through a fistula cava-aorta to deploy the valve [6]. In our case, we decided to use the Brockenbrough needle. This allowed us, with the help of pressure measurement in the tip of the needle and the image fusion, not only to know when we entered the abdominal aorta, but also having a better support. It was very important to choose a zone without calcium and avoiding iliac bifurcation and renal arteries to proximal. The next steps were the usual, and finally, the closure of the fistula aortic vein was made and there was not access complications. In the literature, there is no reference to transcaval access with the use of Brockenbrought needle.
No comments:
Post a Comment